
Low Progesterone Causes, Symptoms, Supplements to Increase Progesterone, and More
Published on
Low Progesterone Causes, Symptoms, Supplements to Increase Progesterone, and More

Low Progesterone Causes, Symptoms, Supplements to Increase Progesterone, and More
If you’re a woman with some hormone-related discomfort, progesterone is the hormone to pay attention to. Low progesterone is linked to many premenstrual and menopausal symptoms. These may be common, but they are neither normal nor healthy. In this article, we’ll empower you with knowledge about progesterone and ways to support it so you can balance your hormones.
What Is Progesterone and Why Does It Matter?
Progesterone is a very important steroid hormone from our ovaries, placenta, and adrenals that plays many big roles in your body, including:
- Helping to maintain your uterine lining to prepare for embryo implantation every cycle
- Supporting a pregnancy
- Interacting with and keeping other hormones, including estrogen and thyroid hormones, in check. For example, estrogen typically stimulates cell growth in the womb and breasts, whereas progesterone inhibits cell growth and promotes maturation.
- Supporting the brain’s relaxation responses, which influences sleep, mood, and overall well-being
- Supporting the health of your cardiovascular system, brain, and bones
- Providing a backbone for other steroid hormones, including cortisol, estrogen, testosterone, and aldosterone
As you get older, both estrogen and progesterone levels gradually decline until menopause. However, progesterone levels drop much faster than estrogen, starting from mid-20s. This is because you have fewer eggs left and also aging ovarian cells produce less progesterone.
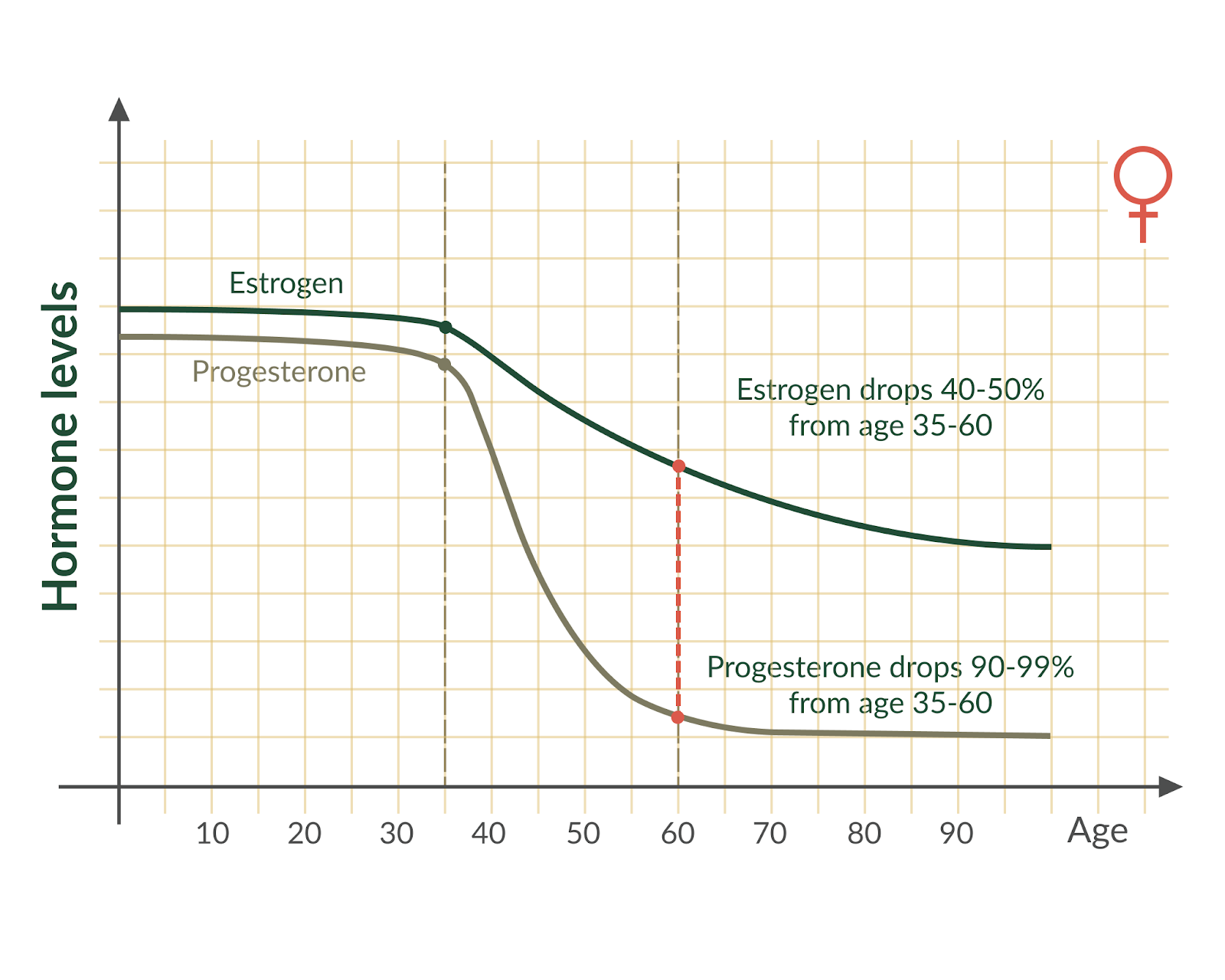
This elevated estrogen relative to progesterone is “estrogen dominance”. This imbalance can contribute to issues like heavy menstrual periods, mood swings, and fatigue. In menopausal women, low progesterone can contribute to hot flashes and night sweats.
Understanding this age-related progesterone decline can be the first step to improving your hormonal well-being. And while you can ask your doctor for prescription progesterone, your progesterone levels and activities are tightly linked to various lifestyle factors. So, you want to first consider diet, lifestyle changes, or even targeted supplementation to support your progesterone levels.
When progesterone functions optimally, your body feels calm and steady. But if levels dip too low, it can throw off everything from sleep patterns to digestion. Understanding progesterone and its role in your body can be a key to feeling your best.
First, let’s look at various symptoms of suboptimal progesterone levels. Then, we’ll discuss progesterone tests, causes of low progesterone, and ways to increase it.
Low or Suboptimal Progesterone Symptoms
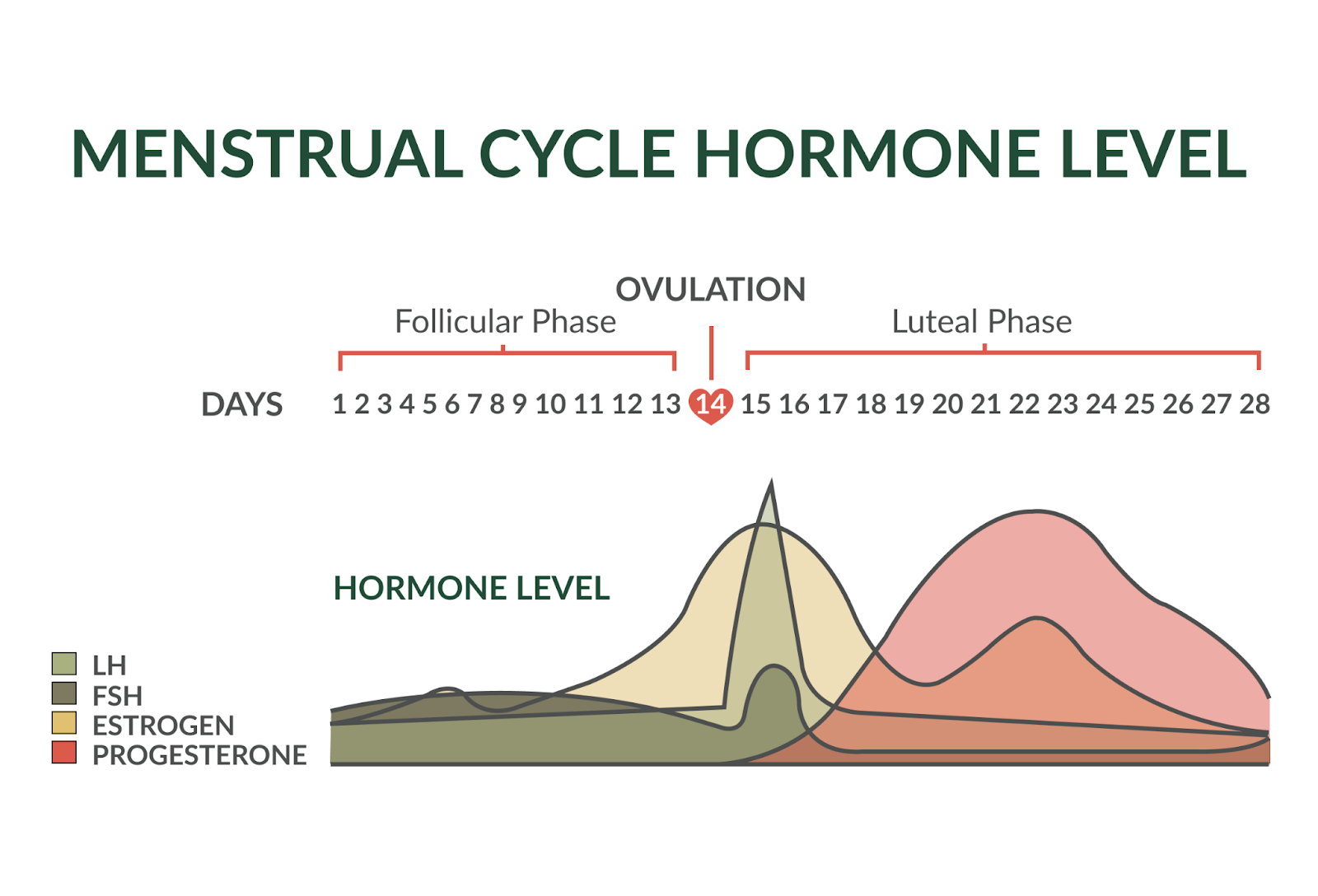
We tend to view the menstrual cycle as two distinct phases – the follicular phase, followed by the luteal phase. Progesterone is the star of this second phase. After ovulation, progesterone levels rise to help prepare your body for a potential pregnancy. If no pregnancy occurs, progesterone levels drop and trigger the onset of your period. This major fluctuation is why some women experience symptoms like mood swings, difficulty sleeping, or bloating during the second half of their cycle in this luteal phase.
If you notice period-related symptoms worsening right before your period, they may be linked to suboptimal progesterone. These can include things like temporary anxiety, cravings, or even digestive issues. Supporting healthy progesterone production can help smooth out these fluctuations and help you feel more balanced during your cycle. It serves as a reminder that your hormones are not just connected to reproduction, but also deeply tied to how you feel every single day. Let’s break down the most common symptoms, and how they might impact you:
Sleep Problems
In women, sleep patterns can fluctuate throughout the menstrual cycle. This is, in large part, because of hormonal changes – specifically progesterone. These shifts can impact both the quality and structure of sleep, with variations in multiple sleep stages, depending on the cycle phase. Let’s look at some of them:
- Women tend to get more deep, slow-wave sleep during the luteal phase of their cycle, because progesterone is calming. Studies find that higher progesterone levels are linked to better deep sleep .
- The progesterone drop right before your period can worsen sleep. Women report waking up more during the night, and having brief awake periods right after falling asleep.
- Progesterone influences REM sleep, the stage of sleep where you dream. It can cause shorter times to enter REM sleep and increase the total amount of REM sleep you get!
- Sleep spindles, specific brain patterns linked to stable sleep, tend to be higher during the luteal phase. Researchers think this might result from the impact of progesterone on certain brain receptors.
If you struggle to fall or stay asleep, it might be related to progesterone. Because of its calming effect, activating receptors in the brain to promote relaxation, sub-optimal progesterone might impact this process. If your levels are low, you may find yourself tossing and turning at night or waking up feeling groggy. The lack of this calming effect can make it harder for your body to transition into deep, restorative sleep.
Mood Issues Towards Feeling More Tension
If you’ve been feeling irritable or unusually tense, low progesterone could be the culprit. Progesterone and its byproducts, like allopregnanolone, normally interact with GABA-A (the calming neurotransmitter) receptors in your brain. Therefore, progesterone partly helps regulate your mood, by balancing out the impacts of other hormones like estrogen and through regulating your stress responses.
When progesterone levels are low, there is less activation through these calming GABA brain pathways, which can increase feelings of tension, irritability, and restlessness.
Low progesterone can also impact the balance between the “fight-or-flight” (a.k.a. sympathetic) and the “rest-and-digest” (a.k.a. parasympathetic) branches of your autonomic nervous system. In the luteal phase when progesterone should dominate, sub-optimal levels might fail to counterbalance stress responses effectively. This can leave you feeling more reactive to stress. Hormonal imbalances might also impact emotional regulation areas in the brain, like the amygdala, which can heighten sensitivity to stress and increase mood issues, such as irritability and tension.
Age-Related Decline in Fertility

As we get older, our progesterone levels naturally decline. This can have impacts on fertility, because this hormone helps prepare your uterine lining for pregnancy. It also helps maintain early pregnancy and prevent contractions. If progesterone levels are low, it can make pregnancy trickier – even if you are otherwise healthy!
Research shows that low progesterone during the luteal phase is linked to lower chances of conception and carrying to term. When progesterone levels are sub-optimal, it can also impact ovulation frequency, even if your menstrual cycles are normal.
While we can’t go back in time or prevent age-related declines in fertility, supporting healthy progesterone levels can set you up for greater success. Optimizing progesterone levels early on in your fertility journey can be a great first step.
Too Heavy or Too Light Cycles
Progesterone regulates the growth of your uterine lining, which means it also affects your menstrual flow. Under normal conditions, estrogen and progesterone work together to maintain balance. Progesterone contributes to the volume of blood loss during your period – when cycles are ovulatory, you typically see heavier bleeding. This is because of progesterone’s role in preparing the uterine lining after ovulation, making it thicker and more developed. Then, when the lining sheds during menstruation, it causes more blood loss. This contrasts with cycles without ovulation, called anovulatory cycles, where progesterone levels are lower, and the lining is less developed.
But, sub-optimal progesterone could also lead to estrogen dominance. Too much estrogen can cause an overgrowth of the uterine lining and contribute to heavier cycles as your body struggles to maintain a consistent rhythm.
If you notice big shifts in the volume of blood loss each month, progesterone might be playing a role.
Cycle-Related Changes in Gut Symptoms

Your gut cells have estrogen and progesterone receptors. These two hormones regulate your digestion and even how healthy your gut flora is.
Ever notice bloating, cramps, or digestive discomfort tied to your cycle? Progesterone affects your gut by:
- Slowing down the movement of food through your stomach and intestines. This helps with nutrient absorption. This can help you feel fuller for longer after having a meal or have fewer bowel movements before your periods.
- Relaxes the esophageal sphincter, the area between your esophagus and stomach.
- Some research even finds that enough progesterone can protect the stomach lining.
- Progesterone also impacts fluid balance in your body.
If progesterone levels are off, you might experience more bloating, constipation, or other gut-related symptoms around your period. You might also notice that your body has more difficulty handling fatty foods. Plus, because of progesterone’s role in fluid balance, low levels might also lead to more fluid retention, weight gain, and breast tenderness.
What Causes Low Progesterone?
Because steroid hormone production starts in the mitochondria, aging is associated with declining mitochondrial function. This may partly explain normal age-related declines in hormones and fertility. Aside from age and certain medical conditions, many women experience symptoms of suboptimal progesterone levels. The following lifestyle factors can further worsen this progesterone decline:
Stress
Progesterone is a precursor to many steroid hormones, including cortisol. During stressful periods, your body prioritizes survival by producing more cortisol at the expense of other steroid hormones. This process is called Pregnenolone Steal. Too much strenuous physical activity and extreme dietary restrictions can also cause pregnenolone steal.
Hormonal Birth Control
There are various types of hormonal birth control, often with a combination of or either estrogen and synthetic progesterone. These work by suppressing ovulation, and thus suppressing your natural hormone production.
Sleep Deprivation

Sleep deprivation disrupts so many hormones, including progesterone. Sleep deprivation increases the risk of anovulation and irregular cycles, as well as reducing both estrogen and progesterone production.
Hormone Disruptors and Xenoestrogens
Every day, we expose our bodies to chemicals known as hormone disruptors . These chemicals can be found in anything from plastics, to personal care products, nonstick cookware, food packaging, and even some foods.
Some of these mimic estrogen functions, while others interfere with progesterone receptors or hormonal functions in some other ways. If you have excess estrogen functions from these chemicals in your body, it can suppress progesterone production.
The big issue with hormone-disrupting chemicals like xenoestrogens is that they tend to sneak into our body, accumulating over time. This makes it harder for your body to maintain optimal hormone levels and functions.
Conclusion: if you struggle with low progesterone, the best course of action is to address your stress levels, optimize your sleep, and minimize hormone disruptors in your life. Some women also choose to switch their birth control in consultation with their doctors. Then, there are some supplement options (see below) that can support hormone balance without suppressing your natural hormone production.
Best Tests for Progesterone Levels and Hormone Balance
You may suspect that you have low progesterone or estrogen dominance, but women’s hormones are complex. One of the easiest ways to determine where your progesterone levels are is through testing. It is important to know that progesterone levels change a lot over the course of your monthly cycle. That can make the timing of testing important. We can measure progesterone through different ways:
Body Temperature, Heart Rate Variability, and Other Measurements
After ovulation, premenopausal women typically have slightly elevated resting body temperature, which is due to progesterone. Some women may also experience a drop in heart rate variability. If your temperature doesn’t rise or stay elevated until your period, it might be a sign that your progesterone is low or you did not ovulate. While many trying to conceive women have tracked their temperature, several wearables nowadays can automatically track your temperature and heart rate variability.
Blood Tests
Hormonal blood tests were developed to diagnose diseases, rather than to pinpoint suboptimal levels. Furthermore, because women’s hormones fluctuate a lot, the normal levels could be too wide to be useful. It’s possible for you to have suboptimal levels but still within normal limits.
Keep in mind also that most steroid hormones in your blood are bound to proteins at any given time, so total serum levels may not reflect levels of functional (free or unbound) proteins.
- During the follicular phase (a.k.a. the first half of your cycle) progesterone levels are naturally low. Around ovulation, progesterone begins to increase, getting up to around 12 ng/mL .
- The luteal phase (second half of the cycle), shows the highest progesterone levels, typically ranging from 1.8 to 24 ng/mL . Progesterone generally peaks between days 21 and 23 of the cycle, making this an ideal window for testing to assess optimal levels.
Functional Hormone Tests and Cycle Mapping
Functional hormone tests like salivary and urine can be another way to better understand your hormonal balance. Most of these panels also measure other steroid hormones, such as pregnenolone, allopregnanolone, cortisol, or metabolites of estrogen and progesterone. Salivary hormones are more representative of the free hormones in the fluids between your cells than your blood hormones. Whereas, urine tests can measure how your body metabolizes hormones.
Because of their less invasive nature and lack of requirement for blood draw, you can map your cycles with these tests. By collecting urine or saliva samples throughout your cycles, you can track fluctuations over the course of your entire cycle.
Therefore, these functional tests can reveal more insights about your health than most hormone blood tests, such as:
- Whether you’re producing the right hormones at the right time
- How your body is metabolizing the hormones or hormone disruptors
- Specific nutrients or supplements you can use to target under-functioning enzymes in your hormone metabolism
- Issues that can interfere with your hormones such as stress and foods
- Whether you’re ovulating consistently or producing enough progesterone at the right time
- Pinpointing specific hormone imbalances
These tests can be especially helpful if you’re experiencing symptoms like irregular cycles, mood swings, or difficulty conceiving, even with normal blood results.
Supporting your body’s natural progesterone production can be a game changer if you want to optimize hormonal health, whether to feel better or improve your fertility. Keep in mind that these tests typically require a doctor’s order and give you a lot of information. Therefore, it’s best to seek out a knowledgeable women’s health naturopathic doctor to order and interpret them for you.
Here, let’s explore natural options to support your progesterone levels.
Supplements and Other Solutions to Increase Progesterone

Vitamin C
While you might think of vitamin C as an important immune nutrient, you may be surprised to know that it is also important for supporting progesterone production! By nourishing the ovaries, this strong antioxidant can help encourage progesterone production during the menstrual cycle. In an animal study, higher concentrations of vitamin C were linked to increased progesterone production and luteal phase activity. This suggests that vitamin C might support your corpus luteum to optimally produce progesterone after ovulation.
Your adrenal glands also rely on vitamin C to manage stress, which indirectly supports healthy hormone levels. The adrenal glands also produce progesterone and are organs with the highest concentration of vitamin C in your body. Vitamin C acts as a cofactor in not just progesterone precursor synthesis, but also for stress hormones. Studies show that women who get enough vitamin C may see a boost in progesterone, leading to better cycle balance and overall hormone health.
Magnesium
Magnesium plays a key role in helping regulate the stress response axis, which is involved in hormone production, including progesterone. Clinical evidence continues to show benefits from magnesium in alleviating symptoms often linked to hormonal imbalances – PMS, bloating, irritability, and fatigue. We tend to see magnesium levels fluctuate with changes in sex hormones across the menstrual cycle. Lower levels of magnesium seem to worsen those late-luteal phase symptoms when progesterone levels are at their peak. Higher levels of progesterone, as we see in the luteal phase, might also deplete magnesium in cells, which could potentially contribute to PMS symptoms. By optimizing magnesium, you might be able to keep some of these issues at bay.
Zinc
Zinc, a small but mighty mineral, is important for helping progesterone work effectively in the body. It plays a key role in how well progesterone binds to receptors in tissues like the uterus, which is critical for hormone function. The right amount of zinc can increase progesterone receptor activity, making it easier for progesterone to carry out its effects.
Zinc also supports the pituitary gland, a key component of the reproductive axis, signaling to your ovaries to release eggs during ovulation – a key step in progesterone production. Finally, zinc also has immune benefits that can encourage a healthy balance between estrogen and progesterone.
B Vitamins, Especially Vitamin B6
Your body requires B vitamins to produce progesterone. One study found that women who consumed more B vitamins from food had a lower risk of developing PMS by 35% .
Vitamin B6, in particular, helps convert cholesterol into progesterone, making it a direct player in hormone synthesis. It also supports the production of serotonin, which can support mood and might even impact PMS symptoms.
B vitamins also help with progesterone production in the adrenal glands. By keeping these systems functioning properly, these nutrients can help ensure your body produces enough progesterone, impact symptoms like mood swings and bloating, and support a more balanced cycle overall!
Vitex
Vitex agnus castus, also known as chasteberry, has been used for centuries to support hormone balance. It works by impacting the pituitary gland – working to increase luteinizing hormone (LH). LH triggers ovulation, boosting progesterone. Vitex is a go-to for many women looking to address PMS symptoms, support regular menstrual cycles, and balance progesterone naturally.
Adaptogens
Stress is an often-overlooked factor when it comes to hormonal health. It can disrupt female reproduction and fertility by impacting the body’s hormonal balance, specifically a pathway known as the hypothalamic-pituitary-gonadal axis which controls reproductive functions. Managing stress and promoting relaxation can help restore normal hormonal balance, and adaptogens like rhodiola can help. When we are chronically stressed, it can suppress ovulation and reduce progesterone levels.
Adaptogens, like rhodiola, can help support the adrenal glands and balance cortisol – a major stress hormone. By balancing your stress response, adaptogens like Stress Guardian and Cycle Care can help foster the perfect environment for your body to produce more progesterone naturally.
Progesterone Supplements and Medications
There are progesterone supplements out there, but keep in mind that progesterone typically doesn’t survive stomach acid. Therefore, you want to get it in micronized form, as a cream, or implantable pellet from a compounding pharmacy. You’ll need a doctor’s prescription as these are considered medications. While supplemental progesterone at the right dose can immediately help with perimenopause and menopause symptoms, you also want to address the root causes and nutrient deficiencies that affect your progesterone levels.
In closing, progesterone is much more than just a reproductive hormone – it is a pillar of your overall hormonal health. From supporting mood and sleep to fertility and digestion, this hormone can influence all aspects of your health and well-being. As you navigate your cycle, keeping progesterone balanced with estrogen and cortisol can help ensure you feel your best. Whether through nutrition, stress management, or targeted supplementation, supporting progesterone can give your body one of the big tools it needs to thrive!
References
- Cable JK, Grider MH. Physiology, progesterone. In: StatPearls. StatPearls Publishing; 2025.
- Peacock K, Carlson K, Ketvertis KM. Menopause. In: StatPearls. StatPearls Publishing; 2025.
- Regidor PA. Progesterone in Peri- and Postmenopause: A Review. Geburtshilfe Frauenheilkd. 2014;74(11):995-1002. doi:10.1055/s-0034-1383297
- Prior JC. Progesterone for treatment of symptomatic menopausal women. Climacteric. 2018;21(4):358-365. doi:10.1080/13697137.2018.1472567
- Mihm M, Gangooly S, Muttukrishna S. The normal menstrual cycle in women. Anim Reprod Sci. 2010;124(3-4):229-236. doi:10.1016/j.anireprosci.2010.08.030
- Thiyagarajan DK, Basit H, Jeanmonod R. Physiology, menstrual cycle. In: StatPearls. StatPearls Publishing; 2025.
- Michener W, Rozin P, Freeman E, Gale L. The role of low progesterone and tension as triggers of perimenstrual chocolate and sweets craving: some negative experimental evidence. Physiol Behav. 1999;67(3):417-420. doi:10.1016/s0031-9384(99)00094-3
- Baker FC, Mitchell D, Driver HS. Oral contraceptives alter sleep and raise body temperature in young women. Pflugers Arch. 2001;442(5):729-737. doi:10.1007/s004240100582
- Parry BL, Mendelson WB, Duncan WC, Sack DA, Wehr TA. Longitudinal sleep EEG, temperature, and activity measurements across the menstrual cycle in patients with premenstrual depression and in age-matched controls. Psychiatry Res. 1989;30(3):285-303. doi:10.1016/0165-1781(89)90020-6
- Lee KA, McEnany G, Zaffke ME. REM sleep and mood state in childbearing women: sleepy or weepy? Sleep. 2000;23(7):877-885.
- Baker FC, Sassoon SA, Kahan T, et al. Perceived poor sleep quality in the absence of polysomnographic sleep disturbance in women with severe premenstrual syndrome. J Sleep Res. 2012;21(5):535-545. doi:10.1111/j.1365-2869.2012.01007.x
- Lee KA, Shaver JF, Giblin EC, Woods NF. Sleep patterns related to menstrual cycle phase and premenstrual affective symptoms. Sleep. 1990;13(5):403-409.
- Armitage R, Yonkers KA. Case report: menstrual-related very short REM latency in a healthy normal control. Sleep. 1994;17(4):345-347. doi:10.1093/sleep/17.4.345
- Ishizuka Y, Pollak CP, Shirakawa S, et al. Sleep spindle frequency changes during the menstrual cycle. J Sleep Res. 1994;3(1):26-29. doi:10.1111/j.1365-2869.1994.tb00100.x
- Kapur J, Joshi S. Progesterone modulates neuronal excitability bidirectionally. Neurosci Lett. 2021;744(135619):135619. doi:10.1016/j.neulet.2020.135619
- Stefaniak M, Dmoch-Gajzlerska E, Jankowska K, Rogowski A, Kajdy A, Maksym RB. Progesterone and its metabolites play a beneficial role in affect regulation in the female brain. Pharmaceuticals (Basel). 2023;16(4):520. doi:10.3390/ph16040520
- Ralevski E, Newcomb J, Pisani E, et al. Progesterone attenuates the stress response in individuals with alcohol dependence and post-traumatic stress disorder – A pilot study. J Dual Diagn. 2024;20(1):39-51. doi:10.1080/15504263.2023.2294989
- Standeven LR, McEvoy KO, Osborne LM. Progesterone, reproduction, and psychiatric illness. Best Pract Res Clin Obstet Gynaecol. 2020;69:108-126. doi:10.1016/j.bpobgyn.2020.06.001
- Ranisavljevic N, Huberlant S, Montagut M, et al. Low luteal serum progesterone levels are associated with lower ongoing pregnancy and live birth rates in ART: Systematic review and meta-analyses. Front Endocrinol (Lausanne). 2022;13:892753. doi:10.3389/fendo.2022.892753
- Labarta E, Rodríguez-Varela C, Mariani G, Bosch E. Serum progesterone profile across the mid and late luteal phase in artificial cycles is associated with pregnancy outcome. Front Endocrinol (Lausanne). 2021;12:665717. doi:10.3389/fendo.2021.665717
- Sanchez EGM, Giviziez CR, Sanchez HM, Agostinho PLS, Barros PS, Approbato MS. Low progesterone levels and ovulation by ultrasound assessment in infertile patients. JBRA Assist Reprod. 2016;20(1):13-16. doi:10.5935/1518-0557.20160004
- Dasharathy SS, Mumford SL, Pollack AZ, et al. Menstrual bleeding patterns among regularly menstruating women. Am J Epidemiol. 2012;175(6):536-545. doi:10.1093/aje/kwr356
- Aguree S, Bethancourt HJ, Taylor LA, Rosinger AY, Gernand AD. Plasma volume variation across the menstrual cycle among healthy women of reproductive age: A prospective cohort study. Physiol Rep. 2020;8(8):e14418. doi:10.14814/phy2.14418
- Alqudah M, Al-Shboul O, Al Dwairi A, Al-U´Datt DG, Alqudah A. Progesterone inhibitory role on gastrointestinal motility. Physiol Res. 2022;71(2):193-198. doi:10.33549/physiolres.934824
- Coquoz A, Regli D, Stute P. Impact of progesterone on the gastrointestinal tract: a comprehensive literature review. Climacteric. 2022;25(4):337-361. doi:10.1080/13697137.2022.2033203
- Rodriguez-Giustiniani P, Rodriguez-Sanchez N, Galloway SDR. Fluid and electrolyte balance considerations for female athletes. EJSS (Champaign). 2021;22(5):697-708. doi:10.1080/17461391.2021.1939428
- Solano ME, Arck PC. Steroids, pregnancy and fetal development. Front Immunol. 2020;10. doi:10.3389/fimmu.2019.03017
- Copinschi G, Caufriez A. Sleep and the ovarian axis. Curr Opin Endocr Metab Res. 2021;17:38-45. doi:10.1016/j.coemr.2021.01.001
- Singleton DW, Khan SA. Xenoestrogen exposure and mechanisms of endocrine disruption. Front Biosci. 2003;8:s110-8. doi:10.2741/1010
- Paterni I, Granchi C, Minutolo F. Risks and benefits related to alimentary exposure to xenoestrogens. Crit Rev Food Sci Nutr. 2017;57(16):3384-3404. doi:10.1080/10408398.2015.1126547
- Gachowska M, Dąbrowska A, Wilczyński B, et al. The influence of environmental exposure to xenoestrogens on the risk of cancer development. Int J Mol Sci. 2024;25(22). doi:10.3390/ijms252212363
- Wang X, Ha D, Yoshitake R, Chan YS, Sadava D, Chen S. Exploring the biological activity and mechanism of xenoestrogens and phytoestrogens in cancers: Emerging methods and concepts. Int J Mol Sci. 2021;22(16):8798. doi:10.3390/ijms22168798
- Charkoudian N, Stachenfeld N. Sex hormone effects on autonomic mechanisms of thermoregulation in humans. Auton Neurosci. 2015;196:75-80. doi:10.1016/j.autneu.2015.11.004
- Schmalenberger KM, Eisenlohr-Moul TA, Jarczok MN, et al. Menstrual cycle changes in vagally-mediated heart rate variability are associated with progesterone: Evidence from two within-person studies. J Clin Med. 2020;9(3):617. doi:10.3390/jcm9030617
- Baker FC, Siboza F, Fuller A. Temperature regulation in women: Effects of the menstrual cycle. Temperature (Austin). 2020;7(3):226-262. doi:10.1080/23328940.2020.1735927
- Owen JA Jr. Physiology of the menstrual cycle. Am J Clin Nutr. 1975;28(4):333-338. doi:10.1093/ajcn/28.4.333
- Mesen TB, Young SL. Progesterone and the luteal phase. Obstet Gynecol Clin North Am. 2015;42(1):135-151. doi:10.1016/j.ogc.2014.10.003
- Wegrzynowicz AK, Beckley A, Eyvazzadeh A, Levy G, Park J, Klein J. Complete cycle mapping using a quantitative at-home hormone monitoring system in prediction of fertile days, confirmation of ovulation, and screening for ovulation issues preventing conception. Medicina (Kaunas). 2022;58(12). doi:10.3390/medicina58121853
- Hills E, Woodland MB, Divaraniya A. Using hormone data and age to pinpoint cycle day within the menstrual cycle. Medicina (Kaunas). 2023;59(7). doi:10.3390/medicina59071348
- Henmi H, Endo T, Kitajima Y, Manase K, Hata H, Kudo R. Effects of ascorbic acid supplementation on serum progesterone levels in patients with a luteal phase defect. Fertil Steril. 2003;80(2):459-461. doi:10.1016/s0015-0282(03)00657-5
- Patak P, Willenberg HS, Bornstein SR. Vitamin C is an important cofactor for both adrenal cortex and adrenal medulla. Endocr Res. 2004;30(4):871-875. doi:10.1081/erc-200044126
- Mumford SL, Browne RW, Schliep KC, et al. Serum antioxidants are associated with serum reproductive hormones and ovulation among healthy women. J Nutr. 2016;146(1):98-106. doi:10.3945/jn.115.217620
- Li W, Zheng T, Altura BM, Altura BT. Sex steroid hormones exert biphasic effects on cytosolic magnesium ions in cerebral vascular smooth muscle cells: possible relationships to migraine frequency in premenstrual syndromes and stroke incidence. Brain Res Bull. 2001;54(1):83-89. doi:10.1016/s0361-9230(00)00428-7
- Habib FK, Maddy SQ, Stitch SR. Zinc induced changes in the progesterone binding properties of the human endometrium. Acta Endocrinol (Copenh). 1980;94(1):99-106. doi:10.1530/acta.0.0940099
- Nasiadek M, Stragierowicz J, Klimczak M, Kilanowicz A. The role of zinc in selected female reproductive system disorders. Nutrients. 2020;12(8):2464. doi:10.3390/nu12082464
- Chocano-Bedoya PO, Manson JE, Hankinson SE, et al. Dietary B vitamin intake and incident premenstrual syndrome. Am J Clin Nutr. 2011;93(5):1080-1086. doi:10.3945/ajcn.110.009530
- Kim K, Mills JL, Michels KA, et al. Dietary intakes of vitamin B-2 (riboflavin), vitamin B-6, and vitamin B-12 and ovarian cycle function among premenopausal women. J Acad Nutr Diet. 2020;120(5):885-892. doi:10.1016/j.jand.2019.10.013
- Höller M, Steindl H, Abramov-Sommariva D, et al. Use of Vitex agnus-castus in patients with menstrual cycle disorders: a single-center retrospective longitudinal cohort study. Arch Gynecol Obstet. 2024;309(5):2089-2098. doi:10.1007/s00404-023-07363-4
- Ivanova Stojcheva E, Quintela JC. The effectiveness of Rhodiola rosea L. preparations in alleviating various aspects of life-stress symptoms and stress-induced conditions—encouraging clinical evidence. Molecules. 2022;27(12):3902. doi:10.3390/molecules27123902